






Advances in Treatments of Essential Tremor
 Date: July 2022
Date: July 2022
Prepared by SIC Member: Han-Lin Chiang, MD
Authors: W.Jeff Elias, MD; Eng King Tan, MD; Joshua Wong, MD; and Michael S. Okun, MD
Editor: Lorraine Kalia, MD, PhD
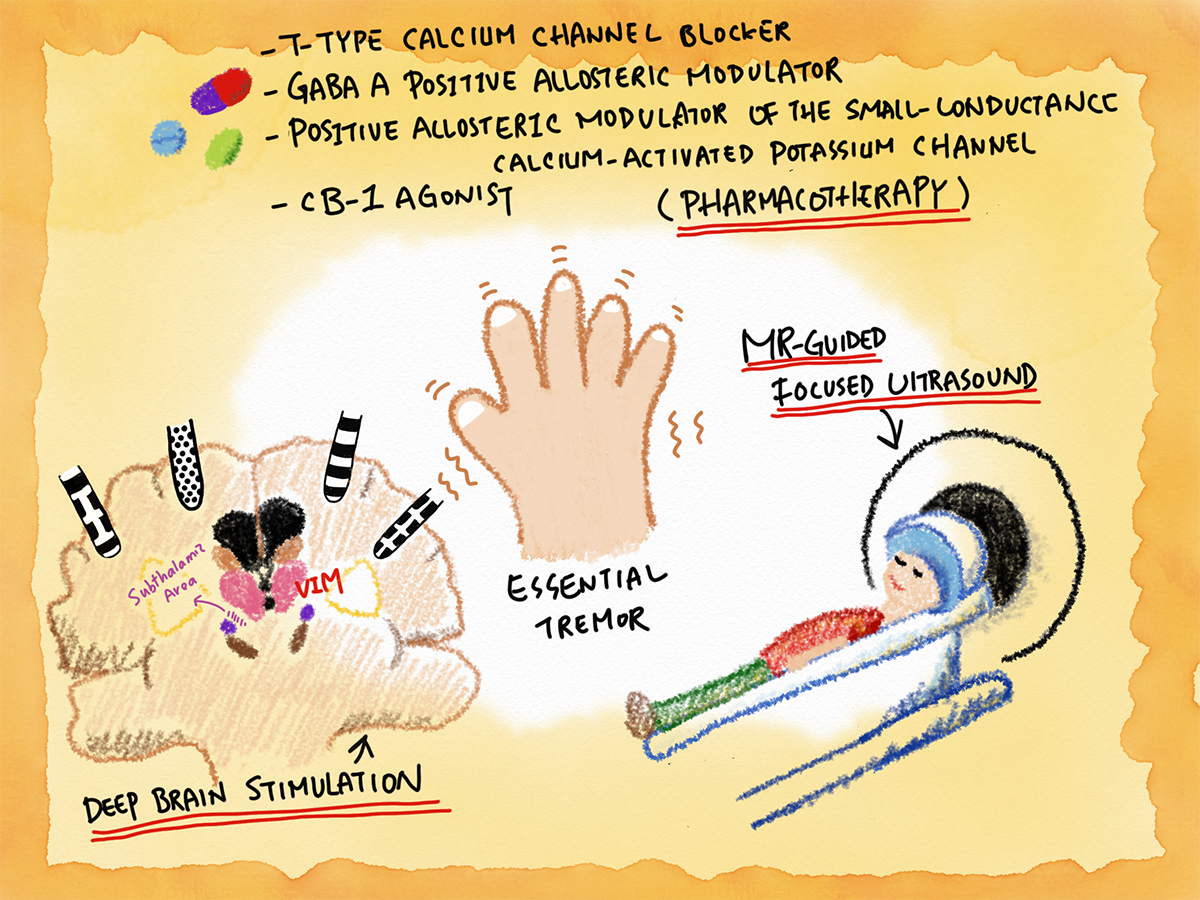
Essential tremor (ET) is one of the most common movement disorders worldwide. According to the International Parkinson and Movement Disorder Society Task Force on Tremor, ET is defined as an isolated tremor syndrome of bilateral upper limb action tremor for at least 3 years, with or without tremor in other locations1. ET tends to progress with age and can eventually become functionally disabling for some patients. Current treatment options include pharmacotherapy, neurostimulation (with deep brain stimulation), and ablative therapies (with radiofrequency, stereotactic radiosurgery, or focused ultrasound) but each has its limitations. Excitingly, new treatment options for ET are emerging. Here we aim to discuss these advances with experts in the field.
1. What are the new drugs in the pipeline for essential tremor and their proposed mechanism of action?
Prof. Eng King Tan:
For pharmacologic agents in essential tremor (ET) patients, propranolol (the only drug approved by the FDA), primidone, and topiramate are considered clinically useful, and alprazolam and botulinum toxin type A possibly useful (MDS evidence based review)1,2. Various benzodiazepines and anticonvulsants are commonly used in clinical practice, most without robust scientific evidence.
Several new investigational drugs have been or currently being investigated2,3. A phase 2 randomized, placebo-controlled trial of CX-8998, a Cav3 T-type calcium channel blocker, improved some aspects of motor performances and activities of daily living in ET patients but the primary end point was not achieved4. Low-threshold burst activity mediated by T-type Ca2 + channels influence the synchronization of neuronal firing and oscillations in the cerebellothalamocortical circuit (implicated ET pathophysiology). PRAX-944 which is a novel T-type calcium channel blocker has been studied in experimental models and human subjects. It reduced tremor without motor effects in rats and in a phase 1 clinical trial the drug was well tolerated in healthy participants5. Cannabidiol modulates CB1 receptor and CB1 agonists have been shown to alleviate tremor in experimental models. However, a randomized controlled, double-blind crossover study did not reduce upper limb tremor in ET patients6. Due to the study design, in which a single oral dose of Cannabidiol or placebo was administered in two experimental sessions performed 2-weeks apart, it isn’t clear whether longer term usage can provide a more positive outcome.
Future clinical trials using investigational drugs should consider both the pharmacokinetic and pharmacodynamic factors and safety profile of the agents, and selection of the most appropriate ET patients based on severity, functional disability, response to previous therapies and possible underlying etiologies.
2. What are the advantages and disadvantages of different deep brain stimulation (DBS) targets for ET? What is the current status of directional leads and closed-loop DBS in ET?
Dr. Joshua Wong and Prof. Michael S Okun:
There are many brain targets to consider when planning DBS for ET. The most common target is the ventralis intermedius nucleus (VIM) of the thalamus. Neuromodulation of the VIM provides overall solid tremor suppression and robust long-term efficacy. The main alternative DBS target for ET is the subthalamic area (STA), a unique area below the thalamus densely packed with axonal fibers. Within the STA lives the prelemniscal radiations and zona incerta. Many DBS centers have explored broadly targeting the STA region or explicitly targeting the prelemniscal radiations and zona incerta within the STA. In general, neuromodulation of the STA offers similar degrees of tremor suppression compared to VIM DBS while possibly requiring less stimulation energy. However, STA DBS may have a higher chance of eliciting stimulation induced ataxia that can be equally debilitating.
Directional leads have provided increased programming flexibility in DBS for ET. However, there has not been a clear benefit to using directional programming over omnidirectional programming in well-placed leads. As such, directional programming may not be a necessary element of the first line programming strategy. On the research side, the directional capabilities of modern DBS leads have been tremendously helpful with adding spatial precision to data collection. For example, by utilizing directional leads during brain electrophysiology recording, we can add a spatial component to the information gathered.
Closed-loop DBS for ET is also advancing rapidly but is not quite mature enough for consumer use. There are many ongoing investigations into the optimal recording paradigm, electrophysiology biomarker and classifier model to produce a system that responds quickly enough to the dynamic temporal nature of tremor in ET. While the emerging data is exciting and promising, further refinement is needed.
3. What are the major determinants and treatment strategies that affect the clinical outcomes and side effects of MR-guided Focus Ultrasound (MRgFUS) for ET? Is bilateral staged MRgFUS thalamotomy a feasible treatment option and how long should we wait?
Prof. Jeff Elias:
The success of MRgFUS thalamotomy for essential tremor continues to improve with increasing experience in the ultrasound community and with advances in the technology. While the great majority of cases are effective and satisfactory to patients with ET, there remain several key variables which must be considered to ensure success:
1. Skull characteristics
Traditionally, neurosurgeons and neuro interventionalists have not paid much attention to the characteristics of the cranium. Transcranial transmission of acoustic energy depends on both the characteristics of the ultrasound wave and the composition of the skull. The skull density ratio (cortical/cancellous) is an assessment of this efficiency, and the FDA approved focused ultrasound thalamotomy for essential tremor in cases where the skull density ratio is higher than 0.4. Cases where the skull density ratio is lower or marginal are at risk for requiring high acoustic energies, prolonged sonication durations, and less sharp focal heating. The size of these lesions varies and can sometimes be larger than expected, obviously with the risk of side effects.
2. Patient selection
Healthy patients with asymmetrical ET respond the best to focused ultrasound thalamotomy. The strongest effect is seen with distal appendicular tremor in the upper limb (hand), but more proximal tremor and even axial tremors can improve. The most functional gains or improvement in quality of life tend to occur when dominant hand tremor is treated. Those patients with premorbid conditions like cerebellar deficits or significant peripheral neuropathy are more prone to bothersome side effects like dysmetria and ataxia.
3. Sonication parameters
There are different ways to achieve a thermal ablation with high-intensity focused ultrasound. The lesioning process can be described with the following formula: Acoustic energy (Joules) = Power (Watts) x Time (seconds). Our group tends to prefer higher ultrasound power and shorter sonication durations, creating a lesion that is sharply demarcated and more reliable to predict. Alternatively, the thermal ablation process could be more of a “slow cook” where the tissue is exposed to lower temperatures for prolonged periods of time. This is often required in cases of lower skull density ratio (less efficient transcranial sonication), and final ablation volumes can vary in shape and size.
4. Experience
The ‘art’ of any stereotactic lesioning procedure involves a balance between lesion size and the risk for a side effect. MRgFUS certainly reflects this as a decision for incremental lesioning can be based on several factors including the clinical response of the tremor, the peak temperature achieved at the target, intraprocedural imaging, and the overall thermal dose delivered. MRgFUS thalamotomy benefits from a closed loop feedback of treatment in which monitoring and incremental lesioning can be performed; but the decision to stop the treatment depends on experience.
Historically, there has been a fear for bilateral thalamotomies as the rates of dysarthria and dysphasia approached 25%, but these cases were primarily performed in an era prior to MRI. Today, bilateral staged thalamotomy may be safe and feasible for ET using FUS lesioning which is extremely precise, continuously monitored, and image guided with MRI. Numerous, single center, clinical trials are underway targeting the VIM in a staged fashion ranging from 5 to 12 months. Bilateral treatments have also been performed targeting the cerebellothalamic tract. A large multicenter trial (NCT04112381) was just completed in 50 subjects where the VIM thalamotomies were staged by at least 9 months, and the results are currently under review with the FDA.
Conclusions
A substantial amount of research is underway to develop new treatments for ET, a common disorder that causes social stigma and functional disability. Pharmacotherapies in the pipeline have varied mechanisms of action, such as T-type calcium channel blockade/modulation (CX-8998 (NCT03101241), PRAX-944 (NCT05021991), JZP385 (suvecaltamide, NCT05122650), NBI-827104 (NCT04880616)) and CB-1 agonism (cannabidiol) as mentioned above. Other drugs in the pipeline include GABA A receptor positive allosteric modulators (SAGE-324 (NCT04305275, NCT05173012, NCT05366751), SAGE-217 (zuranolone, NCT02778781)) and positive allosteric modulators of the small-conductance calcium-activated potassium channel (CAD-1833 (rimtuzalcap, NCT03688685)). All of the clinical trials testing these agents are either still under recruitment or have just completed their phase II trial. Hopefully, some agents will successfully advance to phase III clinical trial in the near future. While both VIM and STA DBS have been quite successful in treating essential tremor, directional DBS leads have the advantage of adding spatial precision to data collection for researchers. As for closed-loop DBS for treating ET, further investigation is still needed before it can be applied to clinical practice. Finally, we are gaining more experience in using MRgFUS to treat ET, and more evidence will soon be available regarding bilateral staged thalamotomy.
References
- Bhatia KP, Bain P, Bajaj N, et al. Consensus Statement on the classification of tremors. from the task force on tremor of the International Parkinson and Movement Disorder Society. Mov Disord 2018;33:75-87.
- Welton T, Cardoso F, Carr JA, et al. Essential tremor. Nat Rev Dis Primers 2021;7:83.
- Ondo WG. Current and Emerging Treatments of Essential Tremor. Neurol Clin 2020;38:309-323.
- Papapetropoulos S, Lee MS, Versavel S, et al. A Phase 2 Proof-of-Concept, Randomized, Placebo-Controlled Trial of CX-8998 in Essential Tremor. Mov Disord 2021;36:1944-1949.
- Scott L, Puryear CB, Belfort GM, et al. Translational Pharmacology of PRAX-944, a Novel T-Type Calcium Channel Blocker in Development for the Treatment of Essential Tremor. Mov Disord 2022.
- Santos de Alencar S, Crippa JAS, Brito MCM, Pimentel AV, Cecilio Hallak JE, Tumas V. A single oral dose of cannabidiol did not reduce upper limb tremor in patients with essential tremor. Parkinsonism Relat Disord 2021;83:37-40.