






![]() VOLUME 27, ISSUE 3 • October, 2023. Full issue »
VOLUME 27, ISSUE 3 • October, 2023. Full issue »

Article of the Year, Movement Disorders Clinical Practice
Have we forgotten what tics are? A re-exploration of tic phenomenology in youth with primary tics
Research suggests that certain features affect clinical presentation in children and youth with tics.
In 1978, the Shapiros published one of the first systematic descriptions of tics in a large sample of youth with Tourette syndrome (TS).1 With other pioneers in the field, they suspected that tic severity increases in childhood2 and declines in late adolescence.3 In recent years, possible differences in presentation of tics by sex have been raised,4,5 like in other neurodevelopmental disorders.6 More recently since the SARS-Cov2 pandemic, the rising phenomenon of functional tic-like behaviors (FTLBs) in youth has enhanced the importance of knowing the typical distribution of tics.
In our study, we aimed to assess the phenomenology of tics in youth and investigate how age, sex, and psychiatric comorbidities influence tic phenomenology. To this end, we have included children and adolescents with primary tic disorders in our registry in Calgary, Canada, since 2017. We examined tic frequency and distribution using the Yale Global Tic Severity Scale (YGTSS), differences between sexes, and changes in tic severity with age and with mental health comorbidities.
203 children and adolescents with primary tic disorders were included (76.4% of males; mean age at first assessment: 10.7 years, 95%CI=10.3–11.1). A total of 49.8% had ADHD, 26.0% had OCD, 28.5% had an anxiety disorder, and 6.6% had depression. At first assessment, the 12 most common tics in youth were simple (Figure 1A). We found that tic-related compulsive behaviors (e.g. tapping, touching, evening-out, etc.) were the most frequent complex motor tics (19%). The most common complex phonic tics were enunciation of syllables (12%) and echolalia (11%). All other complex phonic tics were uncommon in our sample, occurring is less than 10% of children. Only 5% of participants had coprolalia, versus 59% in the cohort of the Shapiros.1 An older age at assessment in the 1978 cohort, changes of diagnostic criteria over the years, and a trend toward the identification of milder cases of TS may explain this difference.
Overall, the distribution of tic frequency and phenomenology has been stable in different studies over the decades.1,4 This suggests that the genesis and manifestation of tics across individuals are rather driven by a common neural factor (a “tic generator,” which would spread across a somatotopic map in the brain) than by environmental factors.7 Our findings emphasize the differences with FTLBs‘ phenomenology, which is critical to have in mind, since management of these conditions is different.
In our sample, females also had slightly higher frequency and intensity of motor tics than males (p=0.032 and p=0.006, respectively), as well as a greater tic-related impairment (p=0.045). In the literature, although findings on sex differences before age 18 varied,4,5 there is accumulating evidence that females may have slightly greater tic severity and tic-related impairment with age.8,9
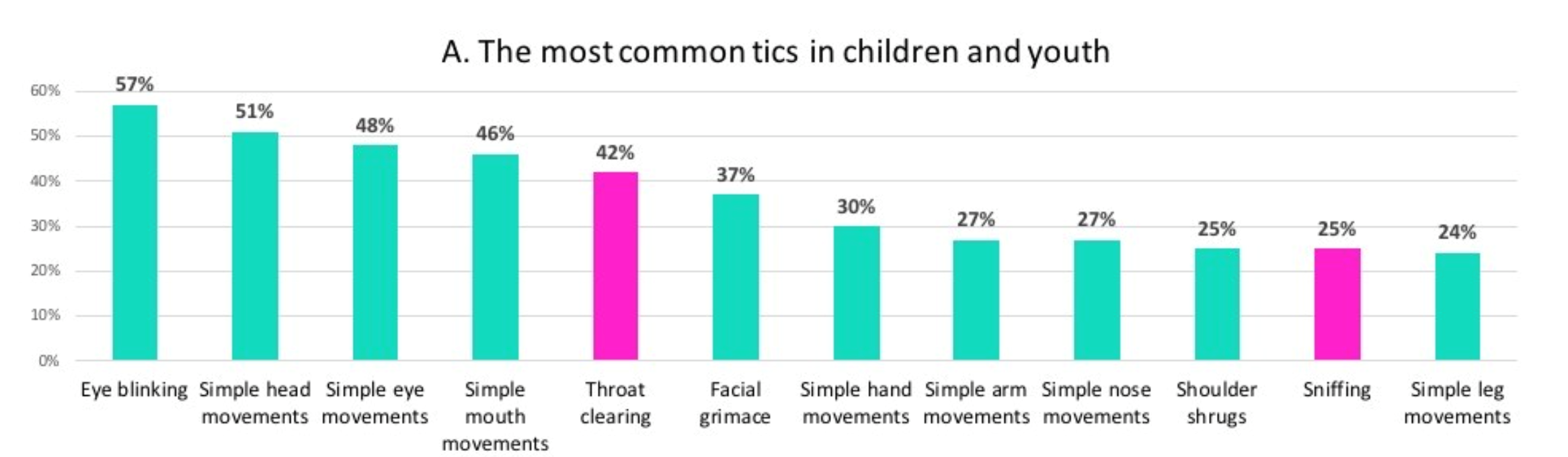
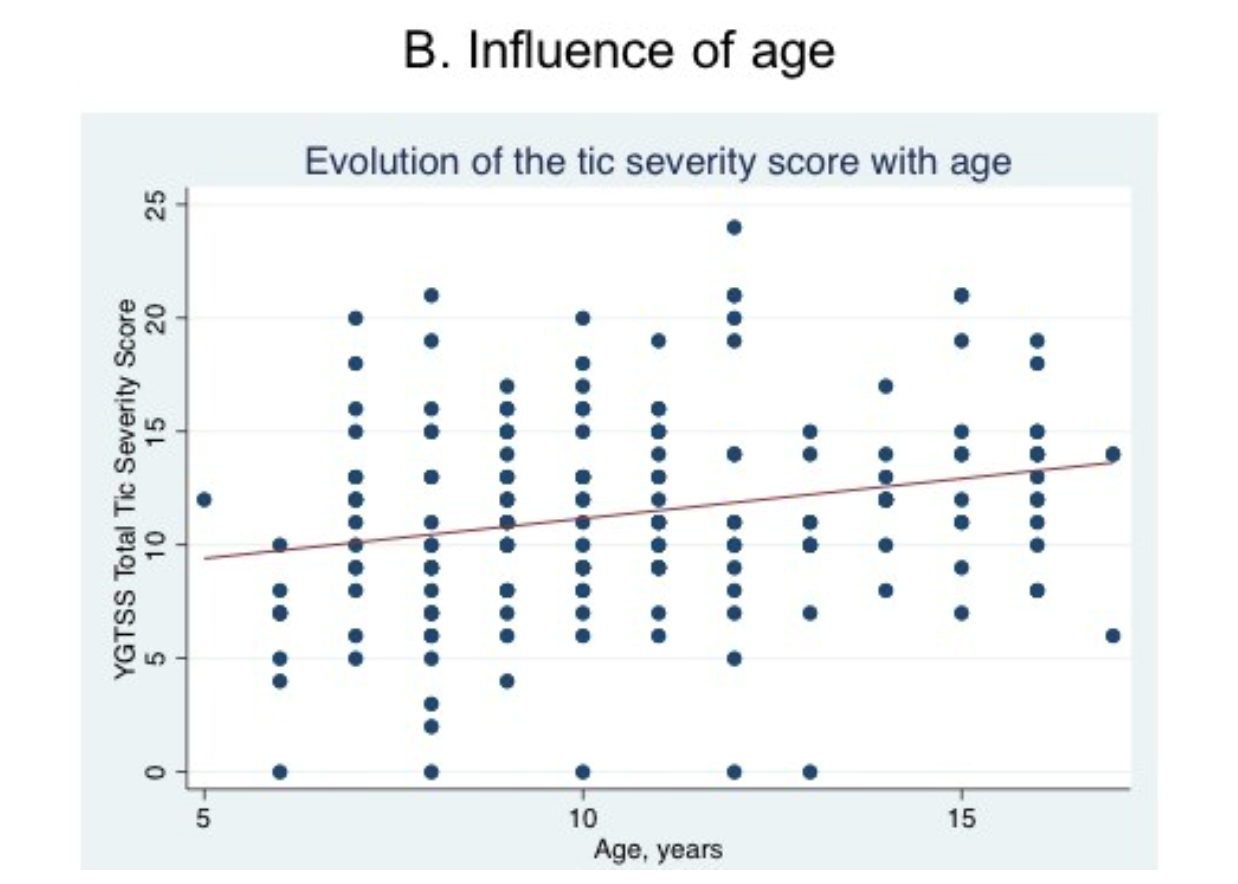
Figure 1: Phenomenology of tics in our sample of children and adolescents with primary tic disorders, and the influence of age and sex.
1A: Prevalences of the twelve most common tics in our sample at first clinical assessment. In green, motor tics; in pink, phonic tics.
1B: Relationship between the Total Tic Severity score (Yale Global Tic Severity Scale) with age (linear regression analysis; coefficient 0.54, p= 0.005).
The Total Tic Severity Score at first clinical assessment increased with age in our cohort (Figure 1B), along with the number, frequency, and intensity of motor tics, but not with their complexity. Our study did not show that the severity of tics decreases in late adolescence, likely due to the fact that tic severity was measured at the first specialty referral, resulting in a selection bias toward more persistent forms in older adolescents.
In our sample, mental health comorbidities were associated with higher motor and phonic tic YGTSS subscores to various extents, as well as with tic-related impairment. This suggests that the association of TS with these comorbidities is associated with greater tic severity, which is consistent with previous findings.10,11
In conclusion, our study suggests that age, sex, and psychiatric comorbidities affect clinical presentation in children and youth with tics. We observed that children and youth with TS typically present with simple motor and/or phonic tics, including simple facial tics. This distribution is very similar to the description of tics in 1978, besides a low frequency of coprolalia in our sample, and contrasts with FTLBs.
Hear from the authors: Listen to an interview on the MDS Podcast.
References
1. Shapiro AK, Shapiro ES, Bruun RD, Sweet RD. Gilles de la Tourette syndrome. Raven Press. 1978;
2. Leckman JF, Zhang H, Vitale A, Lahnin F, Lynch K, Bondi C, et al. Course of Tic Severity in Tourette Syndrome: The First Two Decades. 1998;8.
3. Groth C, Mol Debes N, Rask CU, Lange T, Skov L. Course of Tourette Syndrome and Comorbidities in a Large Prospective Clinical Study. Journal of the American Academy of Child & Adolescent Psychiatry. 2017 Apr;56(4):304–12.
4. Baizabal-Carvallo JF, Jankovic J. Sex differences in patients with Tourette syndrome. CNS Spectr. 2022 Feb 16;1–7.
5. the EMTICS collaborative group, Garcia-Delgar B, Servera M, Coffey BJ, Lázaro L, Openneer T, et al. Tic disorders in children and adolescents: does the clinical presentation differ in males and females? A report by the EMTICS group. Eur Child Adolesc Psychiatry [Internet]. 2021 May 4 [cited 2022 Jul 1]; Available from: https://link.springer.com/10.1007/s00787-021-01751-4
6. Meoni S, Macerollo A, Moro E. Sex differences in movement disorders. Nat Rev Neurol. 2020 Feb;16(2):84–96.
7. Ganos C, Bongert J, Asmuss L, Martino D, Haggard P, Münchau A. The somatotopy of tic inhibition: Where and how much?: The Somatotopy Of TIC Inhibition. Mov Disord. 2015 Aug;30(9):1184–9.
8. Lewin AB, Murphy TK, Storch EA, Conelea CA, Woods DW, Scahill LD, et al. A phenomenological investigation of women with Tourette or other chronic tic disorders. Comprehensive Psychiatry. 2012 Jul;53(5):525–34.
9. Lichter DG, Finnegan SG. Influence of Gender on Tourette Syndrome Beyond Adolescence. Eur psychiatr. 2015 Feb;30(2):334–40.
10. Mol Debes NMM, Hjalgrim H, Skov L. Validation of the Presence of Comorbidities in a Danish Clinical Cohort of Children With Tourette Syndrome. J Child Neurol. 2008 Sep;23(9):1017–27.
11. Rizzo R, Gulisano M, Martino D, Robertson MM. Gilles de la Tourette Syndrome, Depression, Depressive Illness, and Correlates in a Child and Adolescent Population. Journal of Child and Adolescent Psychopharmacology. 2017 Apr;27(3):243–9.
Read more Moving Along: