






![]() VOLUME 30, ISSUE 1 • March 2026. Full issue »
VOLUME 30, ISSUE 1 • March 2026. Full issue »

Session Highlight: 2026 PAS Congress
Integrated care in movement disorders: Multidisciplinary models for better outcomes
Practical tools and approaches to address a ‘new era’ of PwP — and the real-world examples where they are already working.
Experts explore how multidisciplinary models enhance patient outcomes, including actionable insights into building collaborative care networks.
Article OverviewJump to: |
Building the transdisciplinary team
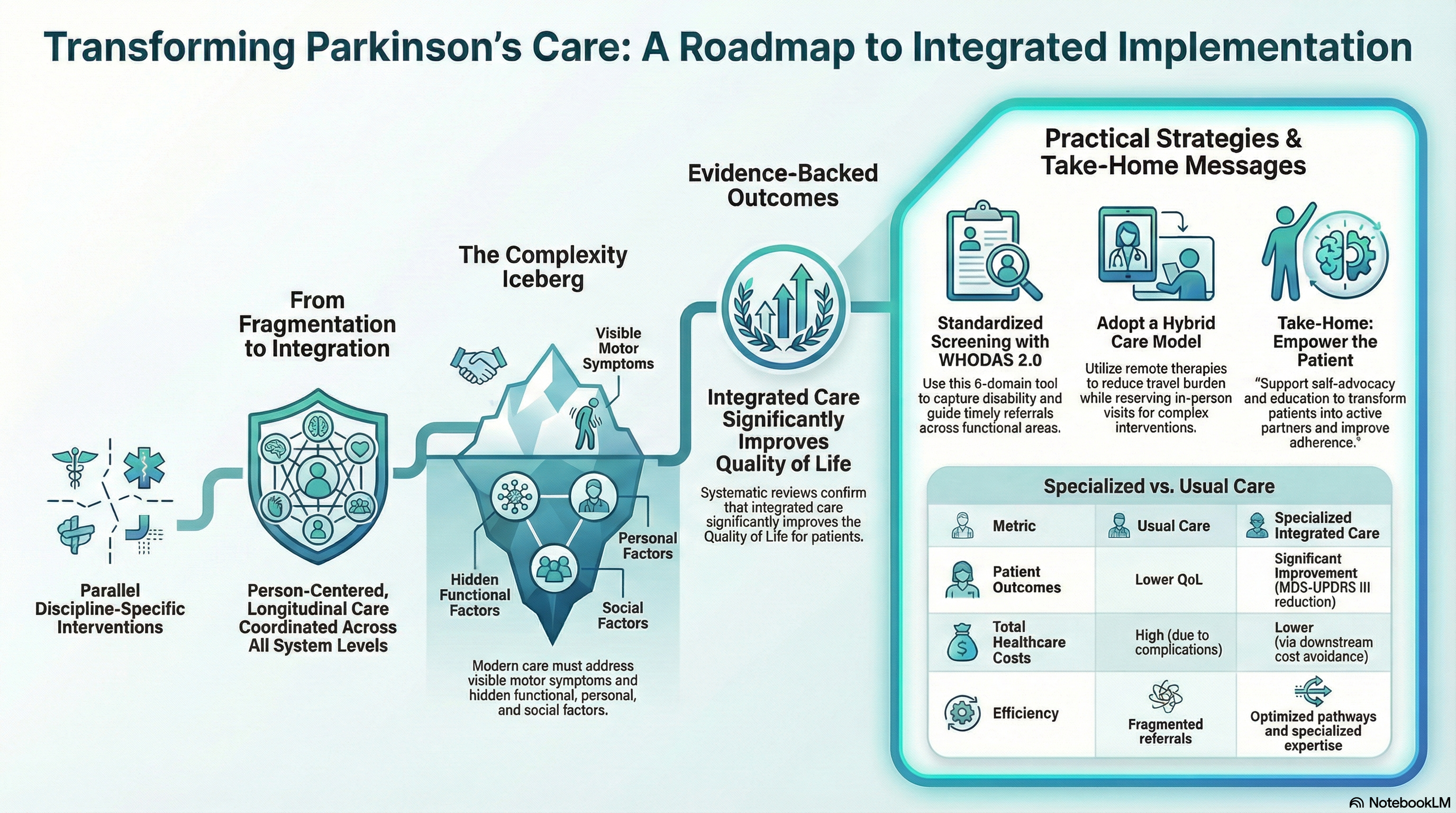
Parkinson’s disease (PD) is a complex, multisystem condition that extends far beyond motor and non-motor symptoms, involving dynamic interactions with personal, social, and environmental factors. This complexity challenges traditional, symptom-centered models of care and highlights the need for integrated approaches throughout the disease trajectory.
A central message of this session was that integrated care is defined by integration and coordination, not by team size. Effective integrated care depends on how well professionals, services, and health system levels are connected through clear referral pathways, shared information systems, and standardized care processes.
Evidence supporting integrated care in PD already exists. A systematic review and meta-analysis conducted by an MDS task force demonstrated that integrated care is associated with better quality-of-life outcomes compared with usual care.
However, the major challenge today lies in barriers to implementation in real-world settings, where most people with PD receive care outside specialized centers. These barriers can be grouped into three categories: |
|
The session highlighted three successful implementation experiences with clear practical lessons: the Kaiser Permanente network-based model, inspired by ParkinsonNet, demonstrated that integrated care can be adapted and scaled across health systems; evidence from ParkinsonNet physiotherapy showed that clinical effectiveness depends on specialized expertise built through structured education combined with high patient caseloads; and the German Parkinson’s Disease Multidisciplinary Complex Therapy (PD-MCT) model illustrated the importance of appropriate referrals for effective interprofessional care.
The key practical strategy to support implementation right now in real-world practice is the early and systematic identification of patient needs. Integrated care must start with recognizing functional, psychosocial, and participation-related needs that often remain undetected by disease-specific instruments. Early identification enables timely and appropriate referral to non-pharmacological interventions.
Tools such as the World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0) support comprehensive functional screening across the full spectrum of functioning. WHODAS 2.0 assesses six key domains: cognition, mobility, self-care, getting along with others, life activities, and participation in society — providing a comprehensive view of disability beyond disease-specific symptoms. The instrument is cross-culturally validated, available in a short 12-item version for routine clinical use, and validated for proxy reporting and remote administration. By systematically identifying unmet functional needs and supporting domain prioritization, WHODAS 2.0 facilitates communication within interprofessional teams and guides therapeutic decision-making, including intervention selection, treatment frequency, and the most appropriate mode of delivery (remote, in-person, or hybrid). This flexibility in care delivery directly supports scalability and sustainability, particularly in settings with limited resources.
In summary, integrated care in PD is achievable in real-world settings when coordination, specialized expertise, and adaptive implementation strategies are prioritized. The focus must shift from idealized team structures to pragmatic solutions that deliver the right care to the right patient, at the right time.
Beyond the clinic: Mental health, quality of life, and the value of community support
I would like to start this topic by keeping in mind how a new image of people with Parkinson’s disease (PwP) has emerged in this decade. The main idea behind this new concept draws our attention to four points: the heterogeneity of the disease, specifically the different percentages found in the age of onset; more exhaustive gender studies in PwP, where males are more frequent only between 60–79 years old; and the variability in disease progression between subjects, for example, fast compared with slow progression. In line with this, the experience of PwP can change throughout the disease and, in many cases, people find a meaningful purpose in their lives despite the disease.
According to the literature, in this new era for PwP, more empathetic approaches have been described around the world, based on multidisciplinary care models that integrate different levels of attention and health care providers. For example, Centers of Excellence of the Parkinson’s Foundation across the United States, the Parkinson’s Day Hospital in Hamburg (Germany), specialized Movement Disorders Clinics in Israel, and the most successful multidisciplinary care model in the Netherlands, ParkinsonNet. All of these models have a “carousel” structure composed of allied health professionals, coordination systems, education for PwP, and health care networks to improve the integral care of PwP.
However, we need to think about these models as part of a puzzle or, as described in a recent paper published by M. Okun, R. Dorsey, and B. Bloem, as a universe: a framework for a new model to deliver care, similar to a solar system. The person with PD is the center of the universe, which includes satellites and planets working together to improve quality of life (QoL) and provide integral care for PwP. But the major elements of this universe are the planets that act as stabilizers of the solar system and provide potential long-term habitats for life. Here is where community-based support (CBS) models are defined.
CBS programs offer social resources and provide a community for PwP, caregivers, and families. The focus of CBS approaches is patient-centered, where the community becomes a therapeutic space. Usually, these programs educate participants about wellness, healthy lifestyles, nutrition, and finances, with a central emphasis on mental health.
To address mental health from the perspective of people living with Parkinson’s disease requires understanding how mental health is defined in order to identify appropriate ways to positively impact their lives. According to the WHO, mental health is “a state of well-being that enables people to cope with the stresses of life, realize their abilities, learn and work well, and contribute to their community.” The relationship with the community is essential because it becomes a driver for creating meaningful social connections.
We now know that mental health in PD is a critical component of integral care. Several studies have reported how poor mental health outcomes in PwP affect quality of life as a consequence of the severity of motor symptoms, pain, fatigue, memory complaints, depression, and anxiety. For this reason, CBS programs allow improvements in physical well-being, strengthen social networks, promote acceptance of the disease through the exchange of experiences between PwP and caregivers, and help diminish stigma.
But what about Latin America? We know that the prevalence of PD in Latin America is growing and that PwP experience psychiatric symptoms, poor mental health outcomes, and higher rates of dependency and early mortality. Because of this, a recent study conducted by PwP, researchers, health care providers, and leaders from Peru, Argentina, Chile, Mexico, Venezuela, Ecuador, El Salvador, Guatemala, Uruguay, and Colombia found that our region has unmet needs related to health systems, specialized allied health professional networks, and limited knowledge about the disease necessary to educate patients about diagnosis, progression, and advanced stages. Other important findings included poor empathy from health professionals when interacting with PwP and limited access to support groups. Despite these barriers, Latin America has resilient populations and several initiatives that work hard to create communities around PwP.
An example of these initiatives is a program called Alianza Parkinson Cali in Colombia. The program was created in 2015 by health professionals, PwP, and caregivers at Fundación Valle del Lili, where the meetings take place. Around 2017, the group of PwP and caregivers requested more frequent meetings based on the success the program had achieved, and then “Sábados en Movimiento” was created, which became a critical point for building a real community-based support program.
With the COVID-19 pandemic, the program faced challenges in maintaining connection with the community, and the group created virtual meetings for everyone. During the pandemic months, the program offered weekly activities including cognitive stimulation, physical activity, and dance classes. After the fear of the pandemic decreased worldwide, new challenges emerged: many PwP did not want to leave their homes, and many developed apathy, depression, or anxiety associated with poor social interaction during the months they spent at home.
With this problem in mind, the group promoted — through social media and word of mouth— the return to in-person meetings at the hospital. However, it was difficult because the group was not the same after COVID-19.
Many challenges still lie ahead, but since 2021 the group has been working to improve strategies to reach more people and encourage participation in regular activities, including weekly tango lessons, educational meetings, caregiver support groups, and directed physiotherapy sessions for all participants on a monthly basis.
After all, we still have many challenges ahead of us, but Latin America continues working to reduce social and demographic barriers for all PwP. We need to work together to: |
|
Palliative care and hospice
Given the palliative care workforce is limited or non-existent in many countries, Movement Disorders clinicians must gain generalist palliative care skills. We have embraced non-motor symptoms for our people with Parkinson’s (PWP) and can expand this to other conditions that we care for. Perhaps the most important aspect of palliative care is changing our focus from the patient to broaden it, including the family (however this looks) in our circle of care. Research demonstrates that PWP who have an engaged caregiver have improved quality of life and less spiritual distress, despite having more severe motor and cognitive symptoms.
Movement disorder neurologists can screen patients for non-motor symptoms, psychiatric symptoms, and spiritual distress. Working in multidisciplinary teams can help increase the supports our patients require and avoid physicians and nurses becoming overwhelmed with multiple care needs of our patients.
While movement disorders clinicians provide care for patients over years to decades, treatment inertia can occur as we focus on scales. Expanding our communication repertoire to ask about values and experience can increase patient engagement with our treatment plans and improve their perception of clinician interactions.
Another barrier to providing effective palliative care can be the “pathologic need to fix” that is common in biomedical training. When we value finding and fixing problems, coping with chronic progressive illnesses can be challenging. We can have discomfort with uncertainty and have feelings of failure, lack of efficacy, and judgment of ourselves and others. Reframing our goal to understanding our patients’ and families’ values and goals and making our best effort to meet them can rejuvenate our practice.
Resources to consider: |
|
Read more Moving Along: